 Article
Article
 27.05.2026
27.05.2026
M.V. Sidorova, Dobrobut Clinic, Kyiv, Ukraine, *Ophthalmology. Eastern Europe*, 2018, Vol. 8, No. 2
Abstract
Introduction.Fixed-dose combinations of antiglaucoma medications allow for the optimization and simultaneous enhancement of the hypotensive effect of eye drops, and the most pathogenetically sound combination is that of a beta-blocker and a carbonic anhydrase inhibitor.
Objective. To evaluate the efficacy and local tolerability of the combination antiglaucoma drug Dorzitima® (2% dorzolamide hydrochloride + 0.5% timolol maleate) in the treatment of patients with glaucoma.
Materials and methods. The study included 45 patients (90 eyes) with newly diagnosed stage II and III open-angle glaucoma. Patients with stage II glaucoma and intraocular pressure (IOP) up to 25 mm Hg were prescribed travoprost as monotherapy, and those with higher IOP were prescribed Dorzitim®. All patients with stage III glaucoma were prescribed a combination of travoprost and Dorzitim®. IOP measurements were recorded after 1 month.
Results and Discussion. In the Dorzitim® group, there was a statistically significant reduction in pressure from 28.45±2.0 mm Hg to 21.05±1.41 mm Hg (p-value <0.05, 38 eyes), which amounted to an average of 26.42%, while in the group receiving travoprost in combination with Dorzitim®, intraocular pressure decreased to 21.09 ± 1.13 mm Hg one month after the start of treatment (p-value <0.05, 34 eyes), with an average reduction of 28.58%.
Conclusion. Dorzitim® is an effective and safe drug for the treatment of glaucoma, both as monotherapy and in combination with travoprost.
Keywords: Dorzit®; medication; monotherapy; travoprost; intraocular pressure; open-angle glaucoma.
INTRODUCTION
Glaucomatous optic neuropathy is a steadily progressive atrophic process in the optic nerve resulting from a disturbance in the pressure gradient between intraocular and intracranial pressure. The success of stabilizing visual function in glaucoma depends on achieving a tolerable pressure—one at which ganglion cell apoptosis stops and atrophy of the retinal and optic nerve fibers does not occur
[1]. Since the value of normal intraocular pressure is individual for each patient, the value of the target pressure in glaucoma is determined based on pachymetry, gonioscopy, and the stage of glaucoma as indicated by visual field defects and nerve fiber loss according to optical coherence tomography data.
Achieving a tolerable intraocular pressure and stabilizing daily fluctuations in intraocular pressure (IOP) help maintain the transport of neurotrophic substances along the axons of ganglion cells, which is essential for preserving the thickness of the optic nerve fibers and results in the stabilization of the visual field for years and even decades after the diagnosis of glaucoma. According to the recommendations of the European Glaucoma Society [2], prostaglandin analogs are the first-line treatment for glaucoma. However, according to the literature, in 35–58% of patients, achieving a tolerable IOP with a single medication is not possible. This is associated with a higher IOP from the outset and, as a rule, stage III glaucoma. Consequently, in one-third of patients, one or two additional antihypertensive medications must be added during the first year of glaucoma treatment to achieve the target pressure [1]. In another 10% of glaucoma cases, IOP cannot be reduced with two medications, necessitating the addition of a third medication. This complicates patient adherence to treatment and “overloads” the ocular surface with the preservatives and buffer solutions contained in each of the antiglaucoma medications separately. The emergence of fixed-dose combinations of antiglaucoma medications has made it possible to optimize and simultaneously enhance the hypotensive effect of eye drops, and the most pathogenetically sound combination is that of a β-blocker and a carbonic anhydrase inhibitor [3].
RESEARCH OBJECTIVE
A Study of the Efficacy in Reducing IOP and Local Tolerability of the Combination Antiglaucoma Medication Dorzitim® (2% dorzolamide hydrochloride + 0.5% timolol maleate) for the Treatment of Patients with Newly Diagnosed Primary Open-Angle Glaucoma.
MATERIALS AND METHODS
The study was a prospective, open-label, observational, single-center trial. The study included 45 patients
(90 eyes) with newly diagnosed stage II and III open-angle glaucoma. Patients with stage I and IV glaucoma were not included in the study, since in stage I, target intraocular pressure can be achieved in all eyes with monotherapy using prostaglandin analogs, and in stage IV, it is impossible to assess changes in visual acuity and visual field. All patients were informed about their participation in the study, signed a consent form, and the study protocol was approved by the clinic’s ethics committee and complies with the principles of the Declaration of Helsinki on the conduct of clinical trials.
The ophthalmological examination included visometry, pneumotonometry, pachymetry, and refractometry using a combined pneumotonometer and ST-1 (Topcon) autorefractometer, as well as perimetry using a Tomey AR ver. 6.1.2 according to the Screening protocol, and biomicroscopy of the anterior and posterior segments of the eye. The open-angle nature of the anterior chamber was confirmed during gonioscopy. The total thickness of the perineural fibers was assessed using the Topcon 3D OCT-2000FA plus (ver. 8.37) optical coherence tomograph according to the 3D Disc protocol (6.0×6.0 mm). Statistical data analysis was performed in SPSS ver. 17 for Windows.
Visual field testing allowed patients to be classified by stage of glaucoma: Stage II in 56 eyes (MD – 3.82±0.87 dB), Stage III in 34 eyes (MD – 7.98±1.27 dB). The mean IOP in patients with newly diagnosed stage II glaucoma ranged from 18 to 33 mm Hg; in this group, travoprost was prescribed as the first-line monotherapy in cases where intraocular pressure did not exceed 24 mm Hg (18 eyes). This is because, according to the Terminology and Guidelines for Glaucoma, travoprost is capable of reducing IOP by 29–31%, which would bring this value down to 16–17 mm Hg. Patients with stage II glaucoma and IOP of 25 mm Hg or higher were immediately prescribed Dorzitim®—a fixed combination of 2% dorzolamide and 0.5% timolol—with the aim of reducing baseline IOP by more than 30%. In all patients with stage III glaucoma, IOP was above 25 mm Hg; they were immediately prescribed two medications—travoprost and Dorzitim® (dorzolamide 2% + timolol 0.5%).
Side effects of the antiglaucoma medications were assessed based on a subjective measure of eye irritation on a 0–3 scale (0 – no irritation, 1 – mild, 2 – moderate, 3 – severe). An objective assessment of conjunctival hyperemia was performed during biomicroscopy and was also rated on a 0–3 scale (0 – no hyperemia, 1 – mild, 2 – moderate, 3 – severe). The distribution of patients by demographic characteristics and stages of glaucoma is presented in Table 1.
| Number of patients | 45 (90 eyes) |
| Distribution by stage | Stage II – 56 eyes Stage III – 34 eyes |
| Age, years (mean±SD) | 73.82±5.84 |
| Gender, M:F | 17:28 |
| Central corneal thickness, μm (mean±SD) | 544.23±18.92 |
| Average deviation (loss of light sensitivity) in the visual field, dB (mean±SD) | Stage II – 3.82±0.87 Stage III – 7.98±1.27 |
| Average nerve fiber thickness, μm (mean±SD) | Stage II – 81.35±11.94 Stage III – 68.52±12.47 |
Note: mean – average, SD – standard deviation.
RESULTS AND DISCUSSION
IOP results for all patients were analyzed after adjustment for central corneal thickness; the data presented in Table 2 reflect these adjusted values. In stage II of newly diagnosed glaucoma, IOP ranged from 18 to 33 mm Hg, which necessitated dividing patients into a travoprost group (18 eyes, baseline IOP up to 24 mm Hg) and a Dorzitim® group (38 eyes, IOP 25–33 mm Hg). Before treatment in the travoprost group, the mean IOP was 22.06 ± 1.45 mm Hg, and after one month, it was 16.56 ± 1.42 (p-value < 0.075). The mean reduction in IOP in the group was 25%, and the significance level was greater than 0.05 (p<0.075) due to the small sample size (18 eyes). In the Dorzitima® group, there was a statistically significant reduction in pressure from 28.45 ± 2.0 mmHg to 21.05 ± 1.41 mmHg (p-value <0.05, 38 eyes), which amounted to an average 26.42% reduction in IOP, although the baseline pressure in these patients was 25 mm Hg and higher. It is noteworthy that in the group receiving travoprost in combination with Dorzitim®, intraocular pressure decreased to 21.09 ± 1.13 mm Hg one month after the start of treatment (p-value <0.05, 34 eyes), which is identical to the result in the Dorzitim® group—21.05 ± 1.41 mm Hg. The baseline IOP in stage III glaucoma was 29.32 ± 1.66 mm Hg, and the average reduction was 28.58%. Thus, the greatest reduction in IOP occurs in the group using three active antiglaucoma medications, however, the degree of IOP reduction in the travoprost + Dorzytim® group is only 2.16% greater than that of the fixed-dose combination of Dorzytim® eye drops (dorzolamide 2% and timolol 0.5%).
| Travoprost (18 eyes, Stage II). Baseline IOP 18–24 mm Hg |
Dorzolamide 2% / timolol 0.5% (Dorzitim®) (38 eyes – Stage II). Baseline IOP 25–33 mm Hg |
Dorzolamide 2% / timolol 0.5% (Dorzitim®) (38 eyes – Stage II). Baseline IOP 25–33 mm Hg |
||||||
| IOP before treatment, mm Hg, mean±SD | IOP after 1 month, mm Hg, mean±SD | p-value | IOP before treatment, mm Hg, mean±SD | IOP after 1 month, mm Hg, mean±SD | p-value | IOP before treatment, mm Hg, mean±SD | IOP after 1 month, mm Hg, mean±SD | p-value |
| 22.06±1.45 | 16.56±1.41 | <0.075 | 28.45±2.0 | 21.05±1.41 | <0.05 | 29.32±1.66 | 21.09±1.13 | <0.05 |
Note: mean – mean, SD – standard deviation, p-value – significance level
An assessment of subjective eye irritation on a 0–3 scale showed that the lowest level of irritation was observed in the Dorzitim® group (31.58%), in half of the patients with travoprost (50%), and in slightly more than half (55.88%) in the group receiving combined treatment with travoprost and Dorzitim®. It can be assumed that the maximum irritation in the latter case is due to the effect of the prostaglandin analog and preservatives from both vials on the stability of the tear film and the conjunctiva’s sensitivity to drying. In the Dorzitima® group, irritation was mild in most patients (26.31%) and moderate in two patients (5.27%). According to patients’ subjective assessments, there was no significant irritation in the Dorzitima® group (Table 3).
An objective assessment of hyperemia on a 0–3 scale revealed virtually identical manifestations of this symptom in the travoprost group and the travoprost group combined with Dorzitim®, at 61.11% and 64.70%, respectively. Such a significant percentage of hyperemia arises due to the negative effect of travoprost, as a prostaglandin—an inflammatory mediator—on the conjunctival vessels and the mucin layer of the tear film. In the Dorzitim® group, hyperemia was observed in only 28.94% of cases and did not exceed a mild degree of manifestation. This is associated with the minimal effect of the β-blocker and carbonic anhydrase inhibitor on the ocular surface and tear film structure (Table 3).
| Subjective assessment | Travoprost, 18 eyes (100%) | Dorzitim® (dorsolamide 2% + timolol 0.5%), 38 eyes (100%) | Travoprost + Dorzitim®, 34 eyes (100%) |
| Irritation, number of eyes (%): −− mild −− moderate −− severe |
9 (50%) 5 (27.77%) 3 (16.67%) 1 (5.55%) |
9 (50%) 5 (27.77%) 3 (16.67%) 1 (5.55%) |
9 (50%) 5 (27.77%) 3 (16.67%) 1 (5.55%) |
| Objective assessment | Travoprost, 18 eyes (100%) | Dorzitim® (dorzolamide 2% + timolol 0.5%), 38 eyes (100%) | Travoprost + Dorzitim®, 34 eyes (100%) |
| Hyperemia, number of eyes (%): −− mild −− moderate −− severe |
11 (61.11%) 2 (11.11%) 6 (33.33%) 3 (16.66%) |
11 (28.94%) 11 (28.94%) 0 0 |
5 (14.70%) 11 (32.35%) 6 (17.65%) |
CLINICAL CASE
This article presents a clinical case of a patient with newly diagnosed open-angle glaucoma. Patient S., 69 years old, presented to the Dobrobut Clinic in Kyiv with complaints of blurred vision in the right eye in the evening. Medical record no. IC 387941. Visual acuity OD=0.2|0.9 c sph – 2.0; OS=0.3|0.9 c sph – 1.5. Pneumotonometry and central corneal thickness: OD 26 mm Hg (484 μm), OS 24 mm Hg (486 μm). The conversion is +4, so the true IOP is 30 and 28 mm Hg.
Biomicroscopy of both eyes shows an identical picture: the eyes are calm, the cornea is clear, the anterior chamber angle is open, and endogenous pigmentation is of moderate severity. In both eyes, the iris pattern is clear; there is no pseudoexfoliation or atrophy of the pigment epithelium. In the lenses, there is early opacification of the posterior cortical layers. In the vitreous body, there is moderately pronounced filamentous degeneration. Fundus findings: The optic disc of both eyes is pale, with clear borders. Optic disc excavation is 0.8 in the right eye and 0.7 in the left eye; there is significant nasal displacement of the vascular bundle, more pronounced in the right eye (Fig. 1).
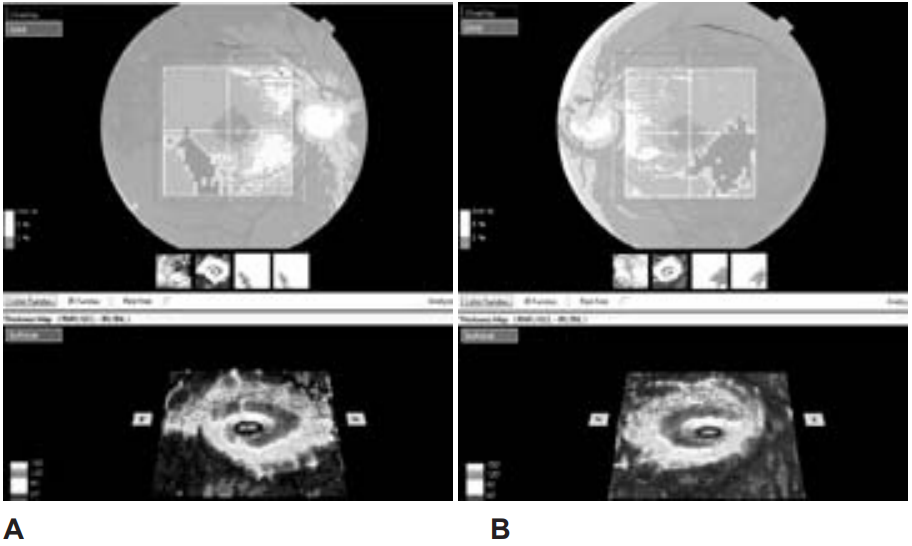
The arteries are narrowed and sclerotic; the veins are wide and moderately tortuous. The macula and peripheral areas in both eyes show no abnormalities.
The ganglion cell layer thickness measurement using the OCT2000FA plus (ver. 8.37) device according to the 3D (V) (NaNxNaNmm) protocol is shown in Fig. 1. Ganglion cell loss (Fig. 1, indicated by arrows) strictly corresponds to scotomas in the visual field (Fig. 2).
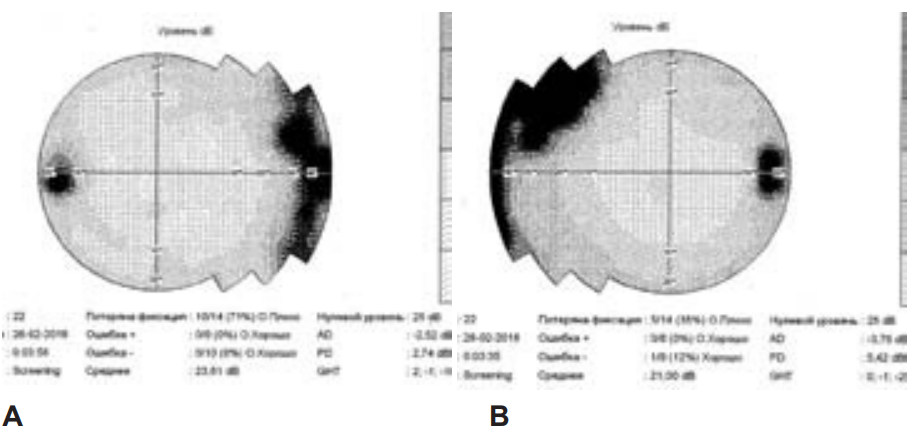
The perimetry was performed using a Tomey AR ver. 6.1.2 device following the Screening protocol. The average defect (AD) in the right eye was 3.76 dB, and in the left eye, 2.52 dB. In the right eye, the formation of a nasal step (indicated by an arrow) and enlargement of the blind spot are noticeable. The data are presented in Fig. 2.
Based on the examination data, the patient was diagnosed with mild myopia and early-stage cataracts in both eyes. Open-angle IIB glaucoma in both eyes. Since the baseline IOP in both eyes exceeded 25 mm Hg, combination therapy was prescribed: travoprost at night, Dorzytim® twice daily in both eyes. IOP monitoring (converted to pachymetry) after 7 days: OD 25; OS 23 mm Hg; after 14 days: OD 22; OS 20 mmHg; after 21 days: OD 21; OS 19 mmHg; after 28 days: OD 21; OS 19 mmHg. Thus, after one month of treatment, IOP decreased by 9 mm Hg (in the right eye from 30 to 21, and in the left eye from 28 to 19), which amounted to 30% for the right eye and 32.14% for the left eye.
The parameters of the optic nerve and the thickness of the perineural fibers were assessed using the 3D Disc protocol (6.0 × 6.0 mm). A large optic disc (over 2 mm) and a wide, deep cup are characteristic of both nerves. However, in the right optic nerve (Fig. 3A), two red sectors of perineural fiber thinning were detected, and in the left optic nerve, three sectors: one at the top and two at the bottom of the nerve (Fig. 3B). Although the visual field corresponds to stage II glaucoma, the cup-to-disc ratio is 0.9 in both optic nerves, and the thickness of the neuroretinal rim is extremely thin, measuring 0.11 in the right eye and 0.04 in the left, which necessitates strict control of IOP and its maximum possible reduction to preserve nerve fibers and the visual field.

CONCLUSION
Dorzytim®, a fixed-dose combination of 1% dorzolamide and 0.5% timolol, demonstrated efficacy in reducing IOP by 26.42% in patients with stage II glaucoma when used as monotherapy, and in combination with travoprost in patients with stage III disease—a 28.58% reduction in IOP. The drug was well tolerated: subjective assessment revealed mild irritation in 31.58% of cases, while objective assessment identified hyperemia in only 28.94% of cases.
REFERENCES
1. Moskalenko V.F., Rykov C.O., Vitovvka O.P., Varyvonchyk D.V. (2010) Scientific justification of the concept of a national strategy for combating glaucoma in Ukraine. Medical Practice, January–February, pp. 121–126.
2. (2017) Terminology and Clinical Guidelines of the European Glaucoma Society on Glaucoma, 4th edition – Chapter 3: Principles and Treatment Options. Supported by the European Glaucoma Society Foundation. Br J Ophthalmol., June; vol. 101(6), pp. 130–195.
3. (2017) European Glaucoma Society. Terminology and Clinical Guidelines on Glaucoma, 4th edition – Chapter 2: Classification and Terminology. Supported by the EGS Foundation. Br J Ophthalmol., May; vol. 101(5), pp. 73–127.