 Article
Article
 30.05.2026
30.05.2026
Based on: Mueller A., Lam I., Kishor K., et al. Secondary glaucoma: toward treatment based on molecular mechanisms. First published: September 5, 2023, https://doi.org/10.1002/wsbm.1628.
Glaucoma is a heterogeneous group of progressive diseases that cause irreversible blindness. Pseudoexfoliation syndrome (PEX) and pigment dispersion syndrome are common causes of secondary glaucoma. These deposits can obstruct the trabecular meshwork, leading to impaired aqueous humor outflow, ocular hypertension, and optic nerve neuropathy.
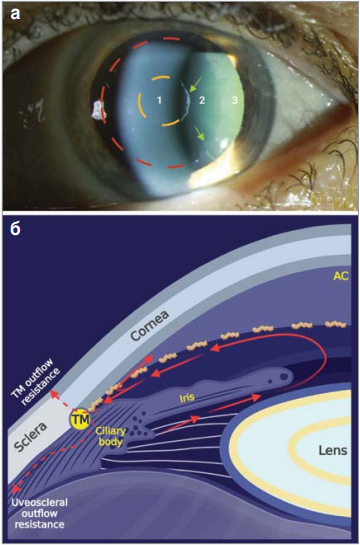
Glaucoma is classified based on the shape of the iridocorneal angle: open-angle (Fig. 1a) or closed-angle (Fig. 1b), as well as by etiology: primary and secondary. The angle formed at the junction of the iris and cornea contains the trabecular meshwork (TM)—a complex, fenestrated structure that serves as a drainage system for AQ. AQ is a clear fluid actively produced by the ciliary processes and fills the anterior chamber of the eye (Fig. 1c). AQ nourishes the cornea, lens, and TC. AQ levels help maintain intraocular pressure (IOP) homeostasis. Inadequate AQ production leads to elevated IOP, causing damage to the optic nerve and progressive vision loss. Initially, glaucoma is characterized by large fluctuations in IOP over a 24 -hour period.
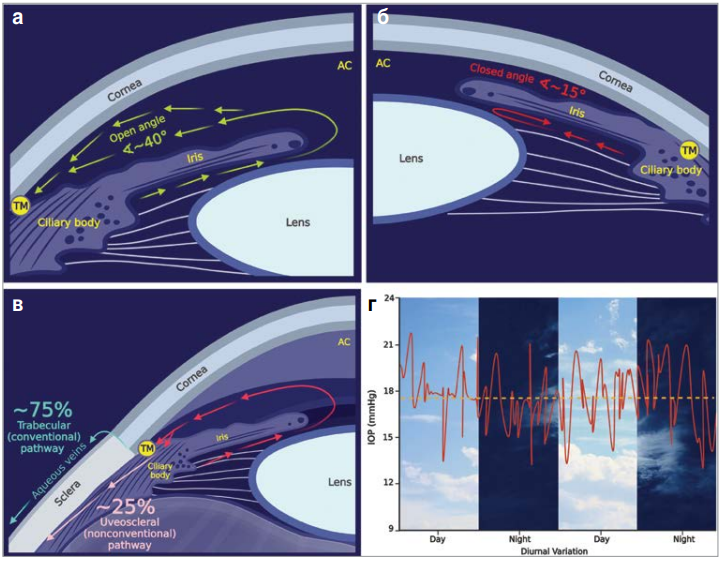
Notes: a) open iridocorneal angle. The anatomical angle (<40°) between the iris and cornea allows AQ produced by the ciliary body to drain from the eye through the trabecular meshwork; b) closed iridocorneal angle. Displacement of the iris and lens causes closure of the iridocorneal angle (<15° or less), which impedes adequate AQ outflow through the TCC; c) physiological pathways of AQ outflow. The trabecular pathway drains 75–90% of AQ through the TCC and aqueous veins. The uveoscleral pathway drains 10–25% of AQ through the pupil and sclera. Both drainage pathways are located beneath the iridocorneal angle; d) significant fluctuations in IOP in the early stages of glaucoma.
Cornea – cornea; open angle – open angle; iris – iris; ciliary body – ciliary body; lens – lens; TM – trabecular meshwork; AC – anterior chamber; closed angle; trabecular pathway; aqueous veins; sclera; uveoscleral pathway; IOP (mmHg); day; night – night; diurnal variation – diurnal variation.
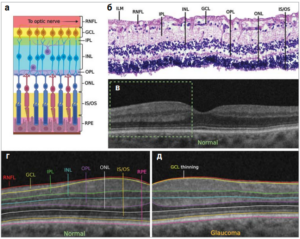
Notes: a) schematic representation of the retinal layers – from top to bottom: retinal nerve fiber layer (RNFL), ganglion cell layer (GCL), inner plexiform layer (IPL), inner nuclear layer (INL), outer plexiform layer (OPL), outer nuclear layer (ONL), inner and outer segments of photoreceptors (IS/OS), retinal pigment epithelium (RPE); b) histological section of the retinal layers stained with hematoxylin and eosin from a healthy eye; c) normal macular OCT image. The area described in Figure 2d is marked in green; d) a close-up of a normal macular OCT image with the retinal layers labeled; e) macular OCT of a patient with glaucoma, demonstrating significant thinning of the GCL.
To optic nerve – to the optic nerve; GCL thinning – thinning of the ganglion cell layer.
Prolonged ocular hypertension has a detrimental effect on the health of retinal ganglion cells (RGCs), which are specialized neurons that transmit visual information from the retina to the brain (Fig. 2) . GCL axons pass through the optic nerve head and extend to the lateral geniculate nucleus in the brain. Non-invasive optical coherence tomography (OCT) can reveal progressive thinning of the neuroretinal layer and enlargement of the optic disc, reflecting the loss of RGC axons, supporting glia, and blood vessels. It is estimated that for every 1 mm Hg increase in mean IOP, the progression of glaucoma increases by approximately 13%.
Peripheral vision is usually affected first, but without treatment, all vision may be lost (Fig. 3a). IOP remains the only known modifiable risk factor for glaucoma. The clinical diagnosis of glaucoma is based on progressive loss of visual acuity on static perimetric maps (Fig. 3b), pallor and cupping of the optic nerve (Fig. 3c), and elevated IOP (Fig. 3d).
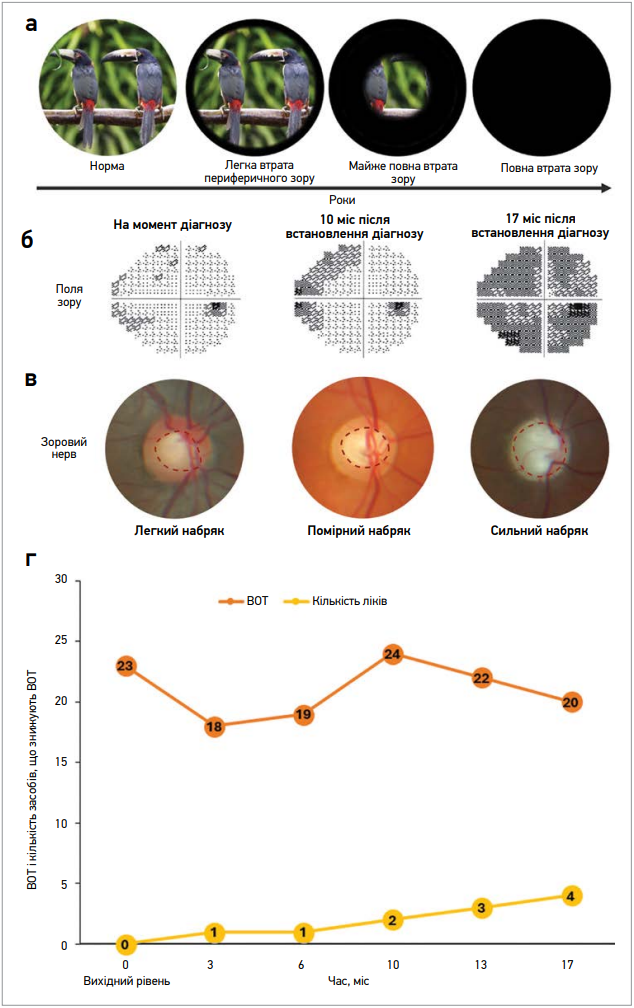
Notes: a) progressive loss of peripheral vision over the years. In the early stages, no changes in vision may be observed. Peripheral vision is affected first. As glaucoma progresses and in the absence of proper treatment, all vision may be lost; b) static perimetry tests for glaucoma at different time points. Gray/black areas represent visual field defects; c) the optic nerve head at different stages of the disease. The optic nerve head (or optic disc) – the site where the axons of the ganglion cells leave the eye to form the optic nerve. Loss of ganglion cell axons and cell bodies causes optic disc edema (red dotted line). An increased cup-to-disc ratio (>0.5) is a sign of glaucoma; d) an increase in the cup-to-disc ratio over time leads to worsening IOP control. The figure shows the patient’s IOP measurements (orange) and the number of IOP-lowering medications they are taking (yellow) over time.
Despite taking multiple medications, IOP may remain above or at the upper limit of normal (the generally accepted range is 10–21 mm Hg).
When the etiology of glaucoma is idiopathic, it is called primary, and if it arises as a result of other diseases, it is considered secondary.
The most common cause of secondary glaucoma is PEX syndrome, an age-related connective tissue disorder characterized by the deposition of loose fibrillar pseudoexfoliative material (PEM) in the extracellular matrix (ECM) of various organs, including the eye (Fig. 4a).
In the eye, PEM can be detected in the structures of the anterior segment and the conjunctiva. PEM and released iris pigment, which are hallmarks of PEX, can accumulate on the trabecular meshwork, increasing resistance to aqueous humor outflow (Fig. 4b). Consequently, IOP rises and gradually leads to glaucomatous optic neuropathy. This pathological process is called pseudoexfoliative glaucoma (PEG). Compared to the most common type of glaucoma, primary open-angle glaucoma (POAG), PEG has a poorer prognosis and is characterized by rapid progression, higher IOP, and a poorer response to medical treatment. In addition, PEXG increases the risk of developing cataracts, complications during cataract extraction, retinal vein occlusion, and lens subluxation.
Notes: a) PEM in the form of a characteristic “bull’s-eye” on the anterior lens capsule; identified as white deposits (green arrows) during slit-lamp examination.
Upon dilation, three zones are visible: the central zone, reflecting the pre-dilated pupil diameter (dotted yellow line); a distinct intermediate zone; and a granular peripheral zone with radial striations (dotted red line); b) increased outflow resistance in PEX. Patchy PEMA deposits in the iridocorneal angle cause inadequate aqueous outflow through the TM and the uveoscleral pathway.
TM – trabecular meshwork; TM outflow resistance – trabecular meshwork outflow resistance; AC – anterior chamber; cornea – cornea; sclera – sclera; iris – iris; lens – lens; ciliary body – ciliary body; uveoscleral outflow resistance – uveoscleral outflow resistance
Pigment Dispersion Syndrome (PDS) is another common cause of secondary glaucoma. PDS typically affects young, nearsighted men. The inheritance of PDS is multifactorial, with both familial and sporadic cases reported. Familial cases demonstrate autosomal dominant inheritance. In PDS, abnormal iridocorneal contact caused by physiological pupil movement and accommodation damages the cells of the iris pigment epithelium and releases pigment. Pigment material is released from the posterior surface of the iris and can then spread throughout the anterior chamber (AC). Pigment granules may settle in the AC, damage surrounding cells, and increase resistance to aqueous humor outflow. Pigmentary glaucoma (PG) occurs when ocular hypertension caused by SDP leads to glaucomatous optic neuropathy. Unlike PEEX, SDP regresses with age, presumably due to age-related changes in accommodation and lens thickness.
Pseudoexfoliative Glaucoma
Epidemiology
The likelihood of developing PEX increases with age; this pattern has been observed in many studies.
Countries with lower temperatures during the summer and winter seasons tend to have a higher prevalence of PEX. Sun exposure, especially when reflected off surfaces such as snow or water, increases the risk of developing PEX. Individuals who spend more time outdoors on average and are exposed to ultraviolet (UV) light throughout their lives are more susceptible to PEX. Higher altitude is associated with an increased risk of developing PECS. Dietary factors also play a role in the development of PECS. Elevated homocysteine levels, which may result from a deficiency in vitamins B6, B12, or folate, are associated with an increased risk of developing PECS.
It has been established that increased folate intake reduces the risk of developing PEXG. In addition, consuming large amounts of coffee and tea increases the prevalence of PEX, likely due to elevated homocysteine levels.
Diagnosis
PEX can be diagnosed based on medical history, dilated pupils, and examination with a slit lamp. Suspected PEX requires gonioscopy, tonometry, visual field testing, and evaluation of retinal nerve fibers using OCT. PEX is an asymmetric, bilateral disorder that may present unilaterally if PEM is distributed unevenly. The bilateral form is typically observed in older patients with higher IOP and a higher prevalence of glaucoma compared to patients with the unilateral form. Unilateral manifestations eventually become bilateral. During examination of the anterior segment, white-gray granular deposits are often visible. A characteristic feature of PEX is pigment loss in the iris sphincter area. Pupil dilation is important for assessing the distribution of PEM on the anterior lens capsule. When the pupil is dilated, three zones delineated by PEM are visible on the anterior lens capsule: a homogeneous central zone reflecting the pre-dilated pupil diameter (may be absent), a distinct intermediate zone, and a granular peripheral zone with radial striations (Fig. 4a).
Patients with PEX may have poor pupil dilation due to fibrotic, ischemic, and atrophic changes in the iris resulting from PEM deposits. During gonioscopy, wavy pigment deposits can be seen in front of Schwalbe’s line (the so-called Sampolezi line). TS demonstrates increased patchy pigmentation (Fig. 4b).
Pathogenesis
PEM is the driving force behind the complex pathological process of PEX/PEXG. Intraocular PEM fibrils are formed by the lens capsule, ciliary body, iris, corneal endothelium, and TS.
PEM is a highly glycosylated, cross-linked, and enzymatically stable glycoprotein/proteoglycan complex. The protein core of PEM consists of the following components of the basement membrane (BM): fibrillin-1, elastin, laminin, and fibronectin, as well as active enzymes such as matrix metalloproteinases (MMPs), clathrin, and lysyl oxidase-like 1 (LOXL1). PEM is resistant to enzymatic degradation by most enzymes, including collagenase, trypsin, pepsin, and papain.
Genetic association studies (GWAS) have identified numerous genetic loci associated with PEX and PEXG, of which LOXL1 has the strongest genetic effect across different populations. LOXL1 is not associated with any other form of glaucoma besides PEXG.
The presence of a single LOXL1 variant does not cause the disease. A significant proportion of unaffected individuals carry the LOXL1 mutation. Environmental stressors play a key role in the pathogenesis of PEX. The complex interaction of numerous molecular elements leads to the formation of a proteolytically stable product (Fig. 5a).
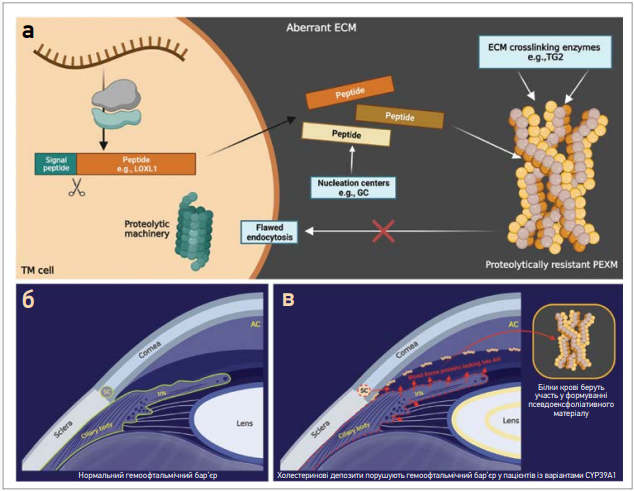
Notes: a) PEX-associated peptides (e.g., LOXL1) are synthesized by the TS cell and secreted into the PM. Nucleation sites, such as GC, provide an optimal environment for peptide aggregation. Regulated cross-linking enzymes, such as TG2, catalyze covalent bonds between these peptides, resulting in the formation of a stable product. Abnormal PMF due to an imbalance of MMPs to TIMPs (not shown) prevents the effective removal of PEM components. Impaired endocytosis prevents the cell from re-absorbing PEM for degradation; b) normal blood-aqueous barrier. The blood-aqueous barrier (green) consists of unpigmented ciliated epithelial cells, epithelial and endothelial cells of the iris, endothelial cells of the iris vessels, and endothelial cells of the inner wall of the Schlemm’s canal; c) an aberrant blood-aqueous barrier (dotted red line) in patients with variants of CYP39A1 loss of function. Abnormally metabolized cholesterol accumulates in non-pigmented cells of the ciliary epithelium, disrupting the blood-aqueous barrier. Blood-borne proteins leak into the aqueous humor and contribute to the formation of ECM.
Aberrant EC – abnormal EC; ECM crosslinking enzymes – ECM crosslinking enzymes (e.g., TG2); nucleation centers – nucleation centers; proteolytic machinery – proteolytic machinery; flawed endocytosis – impaired endocytosis; TM cell – trabecular meshwork cell; proteolytically resistant PEXM – proteolytically resistant pseudoexfoliative material; cornea – cornea; open angle – open angle; iris – iris; ciliary body – ciliary body; lens – lens; TM – trabecular meshwork; AC – anterior chamber; SC – Schlemm’s canal.
Aberrant EC – aberrant endothelial cells, ECM crosslinking enzymes – ECM crosslinking enzymes (e.g., TG2), nucleation centers – nucleation centers, proteolytic machinery – proteolytic machinery, flawed endocytosis – impaired endocytosis, TM cell – trabecular meshwork cell, proteolytically resistant PEXM – proteolytically resistant pseudoexfoliative material, cornea – cornea, open angle – open angle, iris – iris, ciliary body – ciliary body, lens – lens, TM – trabecular meshwork, AC – anterior chamber, SC – Schlemm’s canal.
MMPs and their inhibitors are involved in the proteolysis of the TS matrix and are critically important in the regulation and maintenance of AQ outflow. In PEX, MMP activity is reduced, whereas the activity of tissue inhibitor of MMP-2 (TIMP-2)—the primary inhibitor of MMPs — is markedly elevated. A complex imbalance between MMPs and TIMPs leads to impaired regulation of the aqueous humor outflow. It should be noted that prostaglandin analogs increase uveoscleral outflow by altering the MMP-to-TIMP ratio in the trabecular meshwork, making them effective first-line treatments for PEXG.
Pigmentary Glaucoma
Epidemiology
PG is the most common non-traumatic cause of glaucoma. From the time of diagnosis, the risk of progression from OCN to PG is 10% after 5 years and 15% after 15 years. In a Latin American study, OCS progressed to PG in 37.5% of the study population after 50.7 months.
OAG affects both men and women, but with a slight predominance of men, especially those with myopia. However, POAG is significantly more common in men (78–93% of cases); approximately 60–80% of patients with OAG and POAG have myopia.
On average, the age at diagnosis of PG ranges between 40 and 50 years. Individuals with a family history of glaucoma have a higher risk of developing SDP, but this does not affect the prognosis.
Diagnosis
The classic diagnostic triad of PG includes radial defects of the iris (RDI), a Krukenberg spindle, and/or severe pigmentation of the anterior chamber. RDI refers to gaps in the iris caused by pigment loss, allowing light to pass through them. If these signs are present, further evaluation can be performed using ultrasonic biomicroscopy and OCT of the anterior segment. Posterior iris curvature and iridociliary contact are characteristic findings on ultrasonic biomicroscopy in cases of SDP. They are most prominent in light-colored eyes; DORs in SDP/PG are arranged in a spoke-like pattern and are typically observed inferonazally. Compared to the “moth-eaten” perizonic DORs in PEX/PEXG, DORs in SDP/PG are mid-peripheral. Asymmetric DORs can cause anisocoria (or unequal pupil size) due to damage to the muscles that dilate the iris. In addition, patients with SDP may also experience acute photophobia, blurred vision, redness, and eye pain, mimicking acute anterior uveitis.
The TS in PG is heavily pigmented. The entire TS may be affected, although the lower segment is usually more pigmented. Compared to the mottled TS seen on PEXG (Fig. 4b), the TS in PG is homogeneous. Pigment deposition may also occur along the Schwalbe line, forming a thin dark line similar to the Sampoalesi line in PEXG. IOP in PG is usually elevated and may rise further during episodes of pigment release.
Pathogenesis
SDP is characterized by abnormal iridolenticular contact, which destroys PER cells and releases melanin granules. As the disease progresses, the entire PER layer is lost.
The melanin pigment secreted in SDP acts as a free radical scavenger and binds toxic cations. Melanin (like PEM in PEX) is resistant to enzymatic degradation.
Melatonin may be beneficial in SDP/PG and PEX/PEXG. Although melatonin is widely known for its role in regulating circadian rhythms, it primarily acts as a free radical scavenger and a broad-spectrum antioxidant. The cascade of free radical scavenging by melatonin is highly effective even at low concentrations.
Melatonin may play an additional role in the regulation of IOP and ocular homeostasis. Like the pineal gland, ocular structures participate in the synthesis of melatonin in a circadian pattern. In normal eyes, IOP fluctuates by 3–5 mm Hg in accordance with the circadian rhythm; melatonin is capable of influencing this fluctuation.
Treatment
Topical prostaglandin analogs (e.g., bimatoprost, latanoprost, travoprost) are widely used agents for lowering IOP in glaucoma. These drugs alter the ratio of MMPs to TIMPs in the aqueous humor, ciliary body, and scleral fibroblasts, increasing uveoscleral outflow.
Typically, eye drop therapy is the first-line treatment for lowering IOP in glaucoma. Due to their potent IOP-lowering efficacy, very low incidence of systemic side effects, and ease of use, prostaglandin analogs are the drugs of first choice. Travoprost was one of the first BAC-containing prostaglandin analogs to be released. Subsequently, a version of the drug without BAC was developed. Some studies have demonstrated no significant difference in the IOP-lowering effect between eye drops containing and those not containing BAC [1] .
During follow-up, IOP is monitored in patients with glaucoma to confirm the efficacy of the eye drops, and visual fields are tested to confirm the presence or absence of visual field defect progression [1].
In a study by K. Inoue, M. Iwasa, et al., changes in IOP and the progression of visual field defects were prospectively evaluated over a 3-year period of monotherapy with BAC-free travoprost eye drops in patients with normal-tension glaucoma. In this trial, IOP decreased by 2.9±2.0 mm Hg, and the rate of IOP reduction was 19.8±17.8% after 3 years of treatment with BAC-free travoprost eye drops. Results may be lower in studies that included subjects with ocular hypertension, open-angle glaucoma, PG, and PEXG; however, no significant difference may be observed if subjects have normal-tension glaucoma. The reason for this is that in this trial, IOP was lower prior to treatment (16.8±2.6 mm Hg) than in patients with ocular hypertension, open-angle glaucoma, PG, or PEXG (24.3–27.4 mm Hg) . No significant difference was found compared to patients with normal-tension glaucoma (14.79–15.0 mm Hg). The results of this study showed that there is no significant difference in the long-term IOP-lowering effect between travoprost eye drops containing and not containing BAC [1].
It is known that IOP reduction and the rate of IOP reduction during long-term use (>6 months) of monotherapy with BAC-containing travoprost eye drops were 2.5–9.3 mm Hg and 16.1–36.6%, respectively. In studies involving subjects with ocular hypertension, open-angle glaucoma, PG, or PEXG, the IOP reduction was 6.3–9.3 mm Hg, which is a high value [2–7].
In a trial by S. Parmaksiz, N. Yuksel et al., the IOP-lowering effect and safety of latanoprost and travoprost, administered every evening, were compared with those of the fixed combination of dorzolamide + timolol (DT), administered twice daily for OAG [7]. This randomized, prospective, controlled study was conducted with 50 patients with GLaG.
Patients were assigned to one of three groups:
At baseline and after 0.5, as well as 1–6 months of therapy, IOP (at 08:00, 10:00, and 16:00), blood pressure, and pulse rate were measured, and an ophthalmological examination was performed. Side effects were recorded during each visit.
The results demonstrated that DT is more effective in lowering IOP than latanoprost and travoprost. Latanoprost and travoprost had similar ocular hypotensive effects in patients with PEXG. All 3 drugs were well tolerated.
The efficacy and safety of latanoprost (compared with travoprost) in patients with exfoliative glaucoma were evaluated in a study by A.G. Konstas, V.P. Kozobolis, et al. [8].
A prospective, controlled, crossover comparison was conducted involving 40 patients with exfoliative glaucoma. It was demonstrated that latanoprost and travoprost significantly reduced 24-hour IOP compared to baseline in exfoliative glaucoma, but travoprost demonstrated greater hypotensive efficacy in the afternoon.
In a randomized, multicenter observational study conducted by A.M. Solish, P.T. DeLucca, et al., 492 patients with ocular hypertension, OCHG, exfoliative glaucoma, and PG. The aim of the study was to compare the IOP-lowering effect, tolerability, and patient-reported outcomes of the fixed-dose combination of dorzolamide/timolol and the concomitant use of brimonidine and timolol after 3 months.
The IOP-lowering effect of the fixed combination of dorzolamide/timolol and the concomitant use of brimonidine and timolol was comparable at 3 of the 4 measured time points. Patient-reported outcomes and the incidence of adverse effects in both treatment groups were similar [9].
The use of melatonin and melatonin analogs, either orally or topically, significantly reduces IOP in both normotensive and hypertensive eyes. In addition, oral administration of melatonin prior to cataract surgery under local anesthesia resulted in anxiolysis, enhanced analgesia, and a reduction in IOP. It has been found that melatonin significantly reduces the expression of β2-adrenergic receptors while simultaneously increasing the expression of α2A-receptors. β2- and α2-adrenergic receptors in the ciliary epithelium regulate IOP production. Melatonin has been studied in combination with other IOP-lowering agents, such as brimonidine, dorzolamide, and timolol; it has been shown that they potentiate the hypotensive effect of these drugs. Melatonin and its analogs can be used as monotherapy or in combination with other pharmacological agents. According to PEX/PEXG, when various environmental insults induce the synthesis of PEM components, nucleation centers, and cross-linking enzymes, melatonin’s ability to effectively neutralize ROS and reduce IOP makes it a potentially beneficial intervention.
Conclusions
The pathogenesis of PEXG and PG is multifactorial. PEM formation is the primary driving factor in the development of PEX/PEXG. Specific environmental stressors, such as UV radiation, promote the synthesis of PEX-associated peptides. When peptides are secreted from anterior segment cells, complex interactions among molecular components lead to the formation of a cross-linked, enzymatically stable glycoprotein/proteoglycan PEM complex. Abnormal cholesterol metabolism may disrupt the blood-aqueous barrier, allowing blood proteins to participate in PEM formation.
SDP is characterized by abnormal iris-lenticle contact, which destroys PER cells and also releases melanin granules. Melanogenesis in the iris and PER melanocytes is aberrant in SDP. Cytotoxic intermediate products of melanogenesis leak from the melanosome, causing the death of melanocytes and PER cells. Melanin and the intermediate products of its synthesis accumulate in the TS, which ultimately leads to resistance to the outflow of BB and PG. Targeted intervention in melanogenesis may potentially reduce the risk of developing PG.
Travoprost may be recommended for PG and OAG. In a study, travoprost demonstrated greater hypotensive efficacy in the afternoon compared to latanoprost.
The fixed-dose combination of dorzolamide/timolol is used for both forms of glaucoma; in OCNG, it demonstrated greater efficacy in lowering IOP than latanoprost and travoprost.
Melatonin is a potent inhibitor of melanogenesis, an antioxidant, and a hypotensive agent. This triad of therapeutic effects makes melatonin a valuable agent for the treatment of SCD/PG. Given its ability to scavenge ROS and lower IOP, melatonin may be an effective adjunctive treatment for OAG/OAG.
Prepared by Olena Kostyuk