

Abstract
Introduction. Effective reduction of intraocular pressure is key to achieving the target pressure. Objective: To evaluate the efficacy of Travinor® (travoprost 0.004%) and the combination antiglaucoma medication Dorzitim® (dorzolamide hydrochloride 2% + timolol maleate 0.5%) in the treatment of primary open-angle glaucoma, as well as to determine the morphometric correlations between optic nerve parameters and central corneal thickness in patients with different stages of primary open-angle glaucoma. Materials and Methods. The study included 45 patients (90 eyes) with newly diagnosed stage I, II, and III open-angle glaucoma. Patients with intraocular pressure (IOP) up to and including 24 mm Hg were prescribed Travinor® as monotherapy, while those with higher IOP were prescribed a combination of Travinor® with timolol 0.5% or Travinor® with Dorzitim® . IOP measurements were taken after one, two, and three weeks. Results. The reduction in IOP on Travinor® monotherapy was 8.54 mmHg over 1 month of observation (from 24.81 ± 0.93 mmHg to 16.27 ± 0.44 mmHg (p < 0.01; n = 17)). Combination therapy with Travinor® and 0.5% timolol showed a reduction in IOP from 28.14 ± 3.37 mm Hg to 19.52 ± 1.94 mm Hg (p < 0.01; n = 19), with an average difference from baseline IOP of 8.62 mmHg, representing a 30.63% reduction. In the group receiving combined treatment with Travinor® and Dorzitim®, IOP decreased from 30.5 ± 1.9 mmHg to 20.62 ± 2.05 mmHg (p < 0.01; n = 9), with a difference from baseline IOP of 32.93%. Conclusions. Travinor® and Dorzitim® are effective and safe medications for the treatment of glaucoma, both as monotherapy and in combination.
Keywords
primary open-angle glaucoma; combination therapy; travoprost; dorzolamide hydrochloride and timolol maleate
Introduction
For many years, glaucoma has remained one of the leading causes of blindness worldwide [1, 2]. This was due to the fact that glaucoma is a complex multifactorial disease caused by genetic predisposition and individual anatomical and functional risk factors [3, 4]. For many years, intraocular pressure (IOP) was the primary indicator relied upon for diagnosis and monitoring of disease stabilization. However, the current understanding of its normal range and limits of variation differs somewhat from that of 20 years ago; in recent years, the concepts of “tolerable” and “target pressure” have emerged [5, 6]. Furthermore, glaucoma is one of those diseases that do not affect the patient’s vision until the third, advanced stage of the disease, and glaucoma detected at this stage often cannot be halted by either eye drops or surgical treatment [7, 8].
Currently, despite the rapid development of methods for optic nerve biomorphometry, IOP remains a dynamic parameter that we can influence with eye drops [8, 10]. Since the early 2000s, scanners have been introduced in ophthalmology to examine the in vivo structure of the optic nerve head and retinal layers, a technique known as biomorphometry using optical coherence tomography and scanning laser polarimetry [7, 9]. This has significantly facilitated our understanding of the process of optic nerve atrophy and, at the same time, has allowed the use of optic nerve and retinal fiber parameters to screen for the progression or stabilization of glaucomatous atrophy. Thus, the concept of target pressure has emerged, which takes on the meaning of a safe pressure in cases when, with stable pressure and minimized daily fluctuations, ganglion cell apoptosis does not occur, leading to further optic nerve atrophy [5, 9].
Study Objective: to investigate the efficacy of IOP reduction using Travinor® and Dorzitim® eye drops, as well as to determine the morphometric correlations between optic nerve parameters and central corneal thickness in patients with different stages of primary open-angle glaucoma.
Materials and Methods
The study group included 23 patients (45 eyes) with newly diagnosed stage I, II, and III open-angle glaucoma. All patients were informed about their participation in the study, signed a consent form, and the study protocol was approved by the clinic’s ethics committee and complies with the principles of the Declaration of Helsinki on clinical trials.
The ophthalmological examination included visometry, pneumotonometry, pachymetry, and refractometry using the ST-1 (Topcon) combined instrument, perimetry using the Tomey AR ver. 6.1.2 instrument according to the Screening protocol, and biomicroscopy of the anterior and posterior segments of the eye. The open-angle nature of the anterior chamber was confirmed by gonioscopy using a Goldman lens. The total thickness of perineural fibers was assessed using a Topcon 3D OCT-2000FA plus optical coherence tomograph (Ver. 8.37) using the 3D Disc protocol (6.0 × 6.0 mm).
Statistical analysis was performed using SPSS ver. 17 for Windows. Visual field testing allowed for the determination of glaucoma stages: Stage I — in 12 eyes (Mean Defect — 3.97 ± 1.75 dB), Stage II — in 17 eyes (MD — 8.98 ± 2.85 dB), Stage III — in 16 eyes (MD — 14.52 ± 2.27 dB) . All patients had newly diagnosed glaucoma; baseline IOP values are presented in Table 1. Newly diagnosed glaucoma at stage I was present in 12 eyes, and the mean IOP was 24.81 ± 0.84 mm Hg; the number of eyes with stage II and stage III disease was nearly equal—16 and 17, respectively. Notably, the initial IOP at these stages differed by an average of only 2.84 mm Hg; that is, in stage II, the baseline pressure in the group was 28.14 ± 3.37 mm Hg, and in stage III, it was 30.98 ± 2.72 mm Hg. This provides a basis for more aggressive IOP reduction as early as stage II glaucoma. All IOP values are presented adjusted for central corneal thickness. The antihypertensive effect of Travinor® in monotherapy and Travinor® ® in combination with Dorzitim® was conducted in groups with different stages of glaucoma.
According to the recommendations of Terminology and Guidelines for Glaucoma, 2017 [2], the first-line drug for glaucoma treatment is a prostaglandin; therefore, patients with baseline IOP up to and including 24 mm Hg were prescribed Travinor® (travoprost) as monotherapy. Since travoprost is capable of reducing IOP by 29–31% [3], the expected mean IOP in this group was 16 mm Hg. This therapy was prescribed in all cases of stage I glaucoma (12 eyes) and in 5 eyes with stage II glaucoma. In cases where the initial IOP was 25–28 mm Hg treatment was initiated with a combination of Travinor® (travoprost) and 0.5% timolol maleate (12 eyes with stage II and 7 eyes with stage III glaucoma) with the aim of reducing IOP by more than 30%. In cases of initial IOP of 29 mm Hg and higher, therapy was initiated with a combination of Travinor® (travoprost) and Dorzitim® (dorzolamide 2% + timolol 0.5%)—with the aim of reducing baseline IOP by more than 35%. This group consisted of 9 eyes with stage III glaucoma.
Pearson’s correlation analysis was performed between data on corneal thickness (μm), total thickness of perineural retinal fibers (μm), and the linear (horizontal) ratio of optic disc cupping to the optic disc. The latter indicator is a ratio rather than an absolute value, making it more suitable for comparative analysis of discs of different sizes. The study included optic discs with an average horizontal diameter of 1.6–1.9 mm.
The statistical significance of differences in IOP values before and after the use of eye drops was assessed using the Student’s t-test, and Pearson’s correlation coefficient was determined using Excel for Windows.
Results and Discussion All patients had newly diagnosed glaucoma; baseline IOP values are presented in Table 1. Monotherapy with Travinor® was administered in 12 eyes with stage I and 5 eyes with stage II glaucoma (n = 17). The reduction in IOP during monotherapy with Travinor® was 8.54 mm Hg over 1 month of observation (from 24.81 ± 0.93 mm Hg
to 16.27 ± 0.44 mm Hg in the group). This reduction in IOP (by 34.42% from baseline) was made possible by the potent active ingredient travoprost 0.004% contained in Travinor®, and initial changes in the trabecular meshwork and Schlemm’s canal of eyes with stages I and II of the disease. None of the patients dropped out of the group; side effects in the form of minor redness, tearing, and pain were observed in 4 eyes. These symptoms were resolved within a week through the use of lubricating eye drops.
| Eye drops used and stage of glaucoma |
Baseline IOP, mm Hg |
IOP after 1 week, mm Hg |
IOP after 2 weeks, mm Hg |
IOP after 3 weeks, mm Hg |
|---|---|---|---|---|
| Travinor® (n = 17) Stage I (12 eyes) Stage II (5 eyes) |
24,81 ± 0,93 | 17,18 ± 0,57 | 16,63 ± 0,48 | 16,27 ± 0,44 p < 0,01 t-test = 1,14 |
| Travinor® + timolol 0.5% (n = 19) Stage II (12 eyes) Stage III (7 eyes) |
28,14 ± 3,37 | 25,88 ± 2,77 | 22,35 ± 1,87 | 19,52 ± 1,94 p < 0,01 t-test = 3,07 |
| Travinor® + Dorzitim® Stage III (9 eyes) |
30,50 ± 1,90 | 28,87 ± 2,42 | 23,43 ± 2,84 | 20,62 ± 2,05 p < 0,01 t-test = 3,35 |
Notes: mean ± SD — mean and standard deviation;
p — significance level;
t-test — Student’s t-test.
Combination therapy with Travinor® and timolol 0.5% included 12 eyes in stage II of the disease and 7 eyes in stage III (n = 17) . During the first week of treatment, IOP in the group decreased slightly—from 28.14 ± 3.37 mm Hg to 25.88 ± 2.77 mm Hg (by a total of 8.03%), which can be explained by sclerosis in the trabecular meshwork and rigidity of the Schlemm’s canal. Subsequently, the rate of IOP reduction was more pronounced, and by the end of the month, the group’s IOP was 19.52 ± 1.94 mm Hg (p < 0.01), with an average difference from baseline IOP of 8.62 mm Hg, representing a 30.63% reduction. Four patients (8 eyes) complained of redness and stinging in the eyes; in all patients, the symptoms subsided after the administration of 0.24% hyaluronic acid eye drops.
| Stage of glaucoma | Corneal thickness, μm |
Linear ratio of excavation to disc |
Total thickness of perineural fibers, μm |
|---|---|---|---|
| Stage I, n = 12 | 507,90 ± 34,75 | 0,52 ± 0,06 | 79,72 ± 8,66 |
| Stage II, n = 17 | 497,52 ± 28,45 | 0,67 ± 0,09 | 60,29 ± 12,08 |
| Stage III, n = 16 | 485,37 ± 25,53 | 0,82 ± 0,10 | 44,93 ± 11,02 |
| Control, n = 30 | 515,49 ± 15,53 | 0,51 ± 0,08 | 83,14 ± 7,94 |
Note: mean ± SD — mean and standard deviation.
In the third group receiving combined treatment with Travinor® and Dorzitim® (9 eyes with stage III glaucoma), IOP decreased slowly and after 2 weeks was 23.43 ± 2.84 mm Hg (23.5% of baseline). After 3 weeks, the mean IOP in stage III glaucoma was 23.62 ± 2.05 mm Hg, and after another week—20.62 ± 2.05 mm Hg (p < 0.01), with a difference from baseline IOP of 32.93%. The use of three active ingredients in two eye formulations has a potentiating effect and also improves patient compliance with treatment [1]. In 2 patients (one eye each with stage III glaucoma), the target pressure was not achieved, and they were referred to an ophthalmic surgeon. It should be noted that in stage III glaucoma, to preserve the viability of optic nerve axons, according to the recommendations of Terminology and Guidelines for Glaucoma, 2017 [2], IOP should be maintained within the range of 17–19 mm Hg, especially considering that gonioscopy revealed marked mixed pigmentation of the anterior chamber angle and a narrow angle profile in half of these patients.
Since all patients underwent optical coherence tomography of the optic nerve, an analysis of certain biomorphometric parameters is of interest. Pearson’s correlation analysis included corneal thickness, total thickness of perineural retinal fibers, and the linear ratio of cup to disc. The data varied depending the stage of newly diagnosed glaucoma. Thus, in stage I, fiber thickness was greatest at 79.72 ± 8.66 μm, which is slightly below normal — 83.14 ± 7.94 μm. In stage II, it was 60.29 ± 12.08 μm, and in stage III, 44.93 ± 11.02 μm, which is 29% of the fiber thickness in a healthy optic nerve. The linear ratio of excavation to disc diameter progressively increased from stage I to stage III; in small discs with a diameter of 1.6–1.7 mm, the excavation ratio in stage III of the disease averaged 0.75, whereas in larger discs it reached 0.98. Pearson’s correlation analysis revealed a positive correlation between the thickness of perineural fibers and the central corneal thickness (+0.54), meaning that patients with a thin cornea exhibit greater thinning of perineural fibers. A negative correlation coefficient (–0.51) was found between corneal thickness and the degree of excavation. Eyes with thin corneas showed greater excavation, which is likely associated with a thinner lamina cribrosa and greater protrusion of fibers in the optic disc toward the orbit—in most of these eyes, stage III glaucoma is observed.
Conclusions
1. In patients with newly diagnosed glaucoma, the regimen for prescribing antihypertensive medications depends on baseline IOP, the stage of glaucoma, and the degree of damage to the optic nerve head and retinal nerve fibers.
2. In patients with stage I and II glaucoma, monotherapy with Travinor® (travoprost) reduced IOP from 24.81 ± 0.93 mm Hg to 16.27 ± 0.44 mm Hg over the course of a month, representing a 34.42% reduction from baseline IOP.
3. The combined use of Travinor® and timolol 0.5% reduced IOP by an average of 8.62 mm Hg in the group, which is 30.63% of the baseline level. This type of treatment is indicated for patients with stage II and III glaucoma with a moderate increase in IOP up to 28 mm Hg, with the aim of reducing the baseline IOP by more than one-third and minimizing its daily fluctuations.
4. For patients with newly diagnosed stage III glaucoma and a baseline IOP above 28 mm Hg, it is advisable to immediately prescribe three active antihypertensive medications in two ophthalmic formulations—Travinor® and Dorzitim® eye drops.
5. A correlation analysis of optic disc morphometric parameters and corneal thickness confirmed findings of more advanced stages of glaucoma and greater nerve fiber thinning in eyes with a thin cornea—less than 485.37 μm.
Clinical Case
Patient M., 56 years old, presented with complaints of decreased vision in the right eye. Upon examination, IOP in the right eye was 30 mm Hg and in the left eye 25 mm Hg; pachymetry was 544 μm. Visual acuity OD = 0.4|0.7 with sph + 1.0 D; OS = 0.3|0.9 c sph + 1.5 D. Diagnosis: mild hyperopia and early-stage cataracts in both eyes. Open-angle type IIIB glaucoma in the right eye and open-angle type IIA glaucoma in the left eye.
Biomicroscopy of both eyes revealed an identical picture: eyes are calm, cornea is clear, anterior chamber angle is open, endogenous pigmentation is of moderate severity. In both eyes, the iris pattern is distinct; there is no pseudoexfoliation or atrophy of the pigment epithelium. In the lenses — there is early opacification of the posterior cortical layers. In the vitreous body — moderately pronounced string-like destruction. On the fundus: the optic disc of both eyes is pale, with clear borders. Optic disc cupping in the right eye is 0.8, in the left is 0.4; significant displacement of the vascular bundle toward the nasal side, more pronounced in the right eye. Arteries are narrowed and sclerotic; veins are wide and moderately tortuous. The macula and peripheral areas in both eyes show no pathology.
Since the initial IOP in the right eye exceeded 28 mm Hg, combination therapy was prescribed: Travinor® at night, Dorzitim® twice daily. For the left eye, Travinor® was prescribed at night in combination with 0.5% timolol twice daily. After one month of treatment, IOP in the right eye decreased by 9 mm Hg to 21 mm Hg, and in the left eye, it decreased by 7 mm Hg to 18 mm Hg.
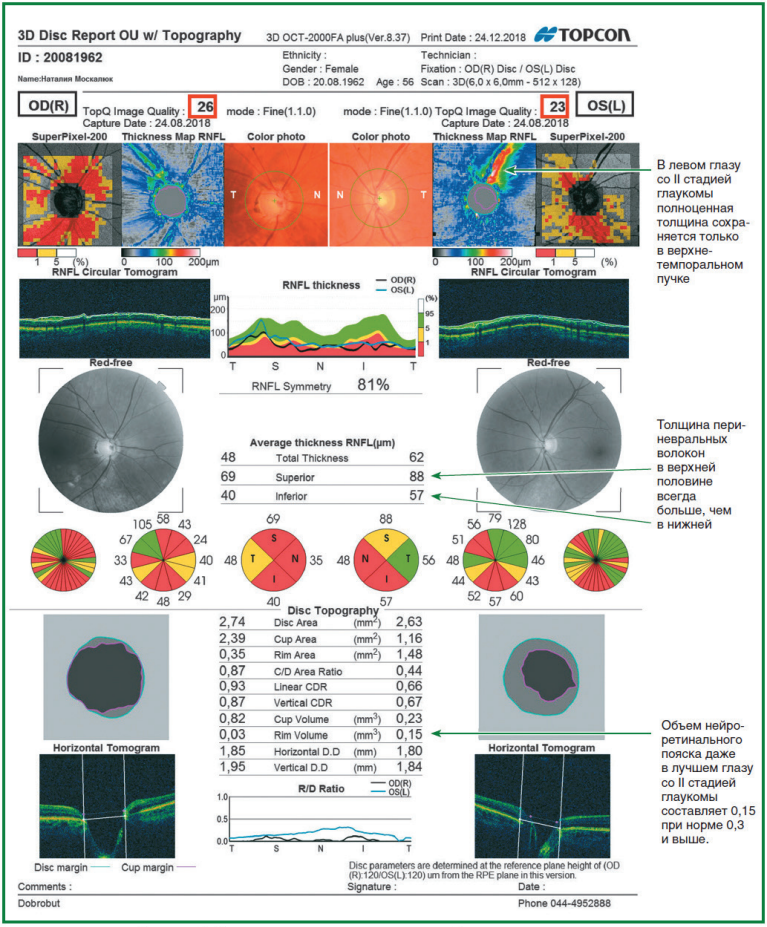
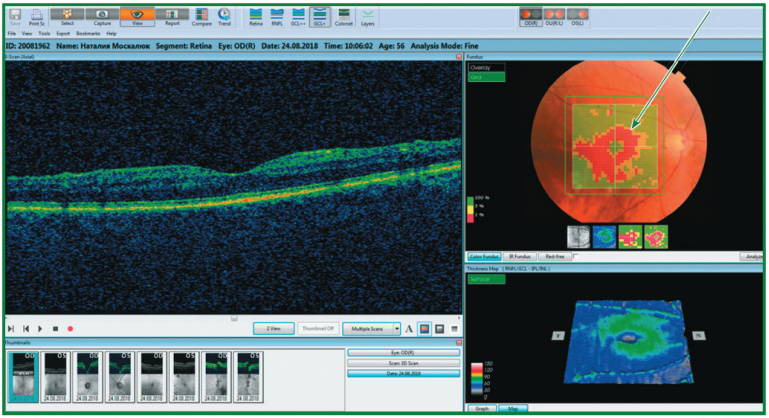
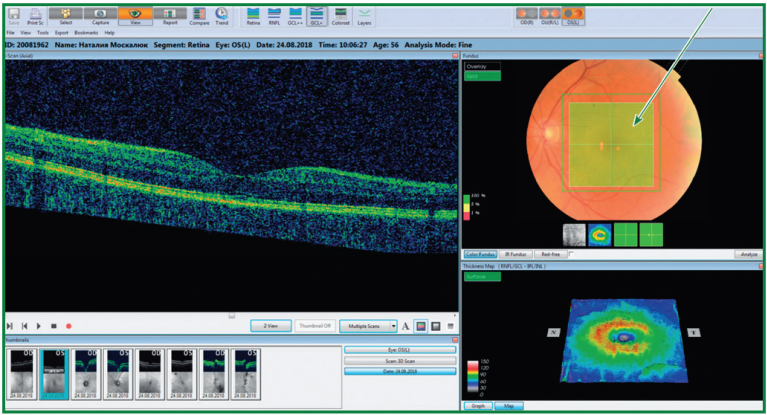
The examination of optic nerve parameters and perineural fiber thickness was performed using the 3D Disc protocol (6.0 × 6.0 mm); the results of the analysis are presented in Fig. 1. The average size is observed in both optic nerves (right 1.85 and 1.95 mm, and the left—1.8 and 1.84 mm horizontally and vertically, respectively), while wide and deep excavation was observed only in the right optic nerve, in which stage III glaucoma was confirmed by perimetry. In the right optic nerve (Fig. 1), seven red sectors of perineural fiber thinning were identified, and in the left—five red sectors, indicating significant apoptotic processes in the nerve fibers of both eyes. The linear cup-to-disc ratio (Linear CDR) in the right eye is 0.93, and in the left eye, 0.66, with a normal value of 0.5. As a result, the rim volume (Rim Volume) even in the better left eye with stage II glaucoma is 0. 15 mm³, compared to a normal value of 0.3 mm³. In the right eye, the rim volume is 10 times smaller than normal and amounts to 0.03 mm³, which suggests strict control of IOP and its maximum possible reduction using Travinor® and Dorzitim® eye drops to preserve nerve fibers and the visual field.
References
1. Alifanova T.A., Gladchenko Y.Y., Chuiko O.L. Disability due to eye disease in Ukraine // Filatov Readings: Scientific and Practical Ophthalmology Conference with International Participation, Dedicated to the 75th Anniversary of the Founding of the V.P. Filatov Institute: Abstracts. — Odessa, 2011. — P. 340.
2. European Glaucoma Society Terminology and Guidelines for Glaucoma, 4th Edition — Chapter 3: Treatment principles and options Supported by the EGS Foundation // Br. J. Ophthalmol. — 2017. — 101 (6). — 130–195.
3. Rikov S.O., Burdei A.V., Zyablitsev S.V., Mogilevsky S.Yu. Predicting the development and progression of primary open-angle glaucoma based on the determination of glutathione-S-transferase gene polymorphisms // Ophthalmol. J. — 2018. — No. 4. — pp. 11–16.
4. World Health Organization. Blindness and visual impairment (accessed Oct. 2017). http://www.who.int/newsroom/fact-sheets/detail/blindness-and-visual-imp…
5. Nesterov A.P. Glaucoma. — Moscow: Medical Information Agency, 2008. — 360 pp.
6. Weinreb R.N., Aung T., Medeiros F.A. The pathophysiology and treatment of glaucoma: a review // JAMA. — 2014. — 311. — 1901–11. [PMID: 24825645].
7. Rikov S.O., Kondratenko Yu.M., Lavrik N.S., Makarenko I.A., Vidiborets S.V. Study of the optic disc condition after two-stage surgical treatment of primary open-angle glaucoma based on the results of scanning laser diagnostic methods // Archives of Ophthalmology of Ukraine. — 2014. — Vol. 2, No. 1. — Pp. 12–19. Available at: http://nbuv.gov.ua/UJRN/aroft_2014_2_1_5.
8. Klyuev G.O., Golovkin V.V. Evaluation of the efficacy of the combination of Dorsamed and timolol 0.5% in the treatment of primary open-angle glaucoma // Ophthalmol. J. — 2016. — No. 2. — Pp. 44–46.
9. Zavgorodnaya N.G., Pasechnikova N.V. A New Look at an Old Problem. — Zaporizhzhia: Orbita-Yug, 2010. — 192 pp.
10. European Glaucoma Society Terminology and Guidelines for Glaucoma, 4th Edition — Chapter 2: Classification and Terminology Supported by the EGS Foundation // Br. J. Ophthalmol. — 2017. — 101 (5). — 73-127. Conflict of interest. None declared.


There are no questions available.